
Anatomy of First Aid: A Case Study Approach
Ronald Bergman, Ph.D.
Peer Review Status: Internally Peer Reviewed
A submarine rendezvoused with its submarine tender and an electrical power line was requisitioned by the submarine to service the submarine while it took on supplies and the crew worked on its nuclear power plant. One of the submariners handling the power line was accidentally electrocuted. Immediately another crewmen moved the Sailor from the power line with a non-conducting wooden pole. A corpsman had been summoned and arrived in time to take over the first aid treatment.


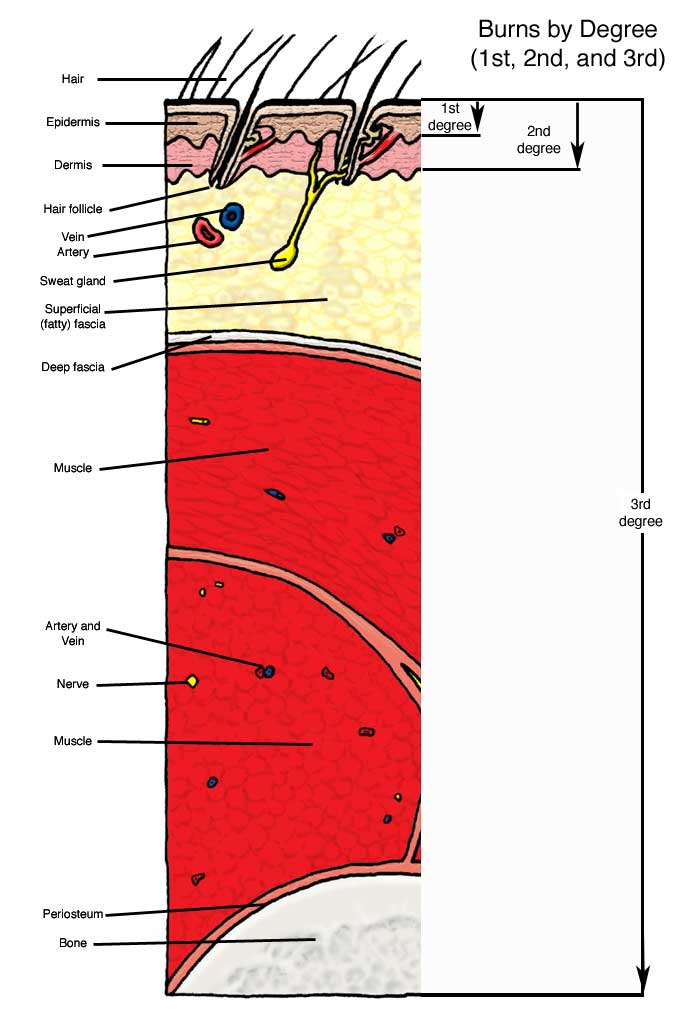
Before discussing first aid given to the submariner, burns, whether caused by flames, electricity, scalding water, friction, radiation or chemicals are described as first-, second- or third-degree burns. The first illustration depicts the tissues effected. A first-degree burn is one involving the epidermis causing erythema (redness) and edema (swelling) but no blisters. A second-degree burn involves the epidermis, the dermis and usually forms blisters that may be the result of superficial or deep dermal necrosis. Burns of this type have epithelial regeneration extending from skin appendages (sweat glands, hair follicles, etc.). A third-degree burn results in the destruction of skin, and may extend into the superficial (fatty) fascia, muscle and bone. Scarring is a consequence of this type of burn.
Returning now to the Sailor with the electric shock; the corpsman knew that electrical burns, even the smallest, are considered third-degree and both an entry and exit burn was possible. The clothing was removed from the areas of both burns, which were quickly, but briefly, cooled with water. A cold wet compress was placed on the wounds followed by clean dry (sterile) dressings. The patient was breathing rapidly, but denied the presence of pain. The absence of pain is typical because nerves are destroyed in the path of the burn. The burns were seen as charred areas about two inches across. The corpsman asked for a blanket to keep the Sailor warm to reduce the possibility of severe shock; his feet were elevated and his vital signs (respiration rate, blood pressure and temperature) were monitored. The corpsman covered the burns with sterile dressings, and the patient was taken to the subtender's sickbay where a naval surgeon took charge of treatment of the burn victim.
Before he left, the corpsman told several interested crewmen that blisters and charred skin would be treated at a later time. In addition he said that butter, household remedies, pain relief medication, ointments or sprays were not to be used for burns of this type and further, if used, may even delay proper healing. The corpsman said that a small third-degree burn might be difficult to recognize if it is located in an area of second- or even first-degree burn skin damage. If there is any doubt, the whole area is treated as a third-degree burn. In addition, because of nerve damage in third-degree burns, a patient must not be allowed to use or put weight on a burned limb, foot or hand.
The knowledgeable medical corpsman continued by explaining to the assembled group the differences between, and treatment for, second- and first-degree burns. First-degree burns are characterized by red skin, mild swelling with or without pain. Second-degree burns are deeper, with red coloration and other skin damage, such as swelling, blisters, oozing or leaking skin, pain greater than 1st degree burns and the possibility of shock . See the first illustration to gain an understanding of the depth of tissue damage in various types of burns. As with other first aid treatments, rapid and proper treatment will reduce the severity of the problem for the patient. With burns of the face, or hot air or hot smoke inhalation assume the possibility of respiratory burns; these require immediate medical attention. Do not remove dead burned tissue and do not open blisters that may form, particularly in second-degree burns. Do not remove clothing that may adhere to the burned area. Do not use home remedies, margarine or butter, ointments or sprays except on the advice of a physician or senior corpsman. Pain relief sprays and ointments can be used on minor or small first-degree burns. Seek the advice of the corpsman for any burns but particularly those of the face, second-degree and extensive first-degree burns. Minor second-degree burns are those small enough to be covered by a small, 3" X 3," sterile dressing but do not involve the face, hands or feet. First aid includes immersion of the burned part under cold running water or if this is impractical, by using cold wet compresses. Continue the cool water treatment until the pain disappears. For second-degree burns of hands, feet, face and/or perineum, e.g., the entire arm or 10 to 15 % of the body, and burns that blister, see the corpsman for advice and additional treatment. Second-degree burns involve deeper areas of the skin that may release fluid from damaged blood vessels that cause blisters. Usual causes are: deep sunburns resulting from prolonged exposure to the sun by Sailors not wearing shirts on outdoor work details, prolonged exposure with hot objects, scalding by hot water or steam, and by flash-burns from inflammable liquids. First-degree burns involve the superficial layers of the skin, which becomes red but not broken or blistered. Pain receptors in the superficial layers of the skin become irritated and produce the perception of pain, which may be intense. Recovery of the skin from the burn is usually quick and complete. Treatment may include cooling with water, aspirin or other analgesics.
The corpsman said he used the "rule of nines" to describe the extent of the burn or area of the burn expressed in percent of the total body surface for an adult. The rule of nines allows that each upper limb is 9%, head and neck is 9%, anterior trunk (chest and abdomen) is 18%, the posterior trunk (back) is 18%, each thigh is 9%, and each leg (not including thigh) is 9%, and the perineum is 1%. Burns need to be treated in the hospital if they are more than 20% of body area, involving a critical area such as face, hands, feet, genitalia, perineum, and major joints, all electrical and chemical burns regardless of size, and smoke inhalation or carbon monoxide poisoning.


The corpsman also discussed chemical burns and stated that exposure to dangerous chemicals must be rinsed from the skin and that contaminated clothing is removed. Water dilutes these substances and flushes them away. No attempts to neutralize the substance should be attempted because greater damage may occur by chemical reaction resulting in additional burning. Frequently encountered products that cause third-degree chemical burns include hydrofluoric acid (rust removers) nitric, sulfuric, phosphoric acids (commercial grade acids) hydrochloric acid (cement and drain cleaners); these chemicals must be used with great care.

Treatment includes removal of contaminated clothes, flushing the affected area with running water for at least 5 minutes. Relieve pain with cool, wet compresses until the corpsman arrives. The corpsman will decide if a naval surgeon is required. He also said that in burns to the face or the inhalation of toxic chemicals; assume a condition of respiratory burns, which require the immediate attention of a physician.

Please send us comments by filling out our Comment Form.
All contents copyright © 1995-2025 the Author(s) and Michael P. D'Alessandro, M.D. All rights reserved.
"Anatomy Atlases", the Anatomy Atlases logo, and "A digital library of anatomy information" are all Trademarks of Michael P. D'Alessandro, M.D.
Anatomy Atlases is funded in whole by Michael P. D'Alessandro, M.D. Advertising is not accepted.
Your personal information remains confidential and is not sold, leased, or given to any third party be they reliable or not.
The information contained in Anatomy Atlases is not a substitute for the medical care and advice of your physician. There may be variations in treatment that your physician may recommend based on individual facts and circumstances.
URL: http://www.anatomyatlases.org/